Ovulation Induction in Chennai
Gentle medication-based protocols to restore regular ovulation and support natural conception in Chennai

Ovulation induction is the entry-level fertility treatment for women who do not ovulate regularly or at all. Using carefully dosed oral medications such as letrozole or clomiphene citrate — and occasionally low-dose injectables — the ovaries are stimulated to develop and release one or two mature eggs. Combined with timed intercourse or IUI, ovulation induction restores the predictable fertile window that irregular cycles disrupt.
Many women with PCOS, hypothalamic dysfunction, or unexplained anovulation conceive with ovulation induction alone, without needing IVF. Dr. Rukkayal designs each protocol based on your specific hormonal profile, ultrasound findings, and body mass index, adjusting doses cycle by cycle to achieve a controlled response. Serial follicular monitoring ensures that the dominant follicle reaches optimal maturity before a trigger injection or natural LH surge prompts ovulation. This close surveillance also prevents excessive follicle development, which could lead to multiple pregnancies or ovarian hyperstimulation. For women who have been prescribed ovulation medications without proper monitoring elsewhere, Dr. Rukkayal provides the structured, evidence-based approach that maximises both safety and success.
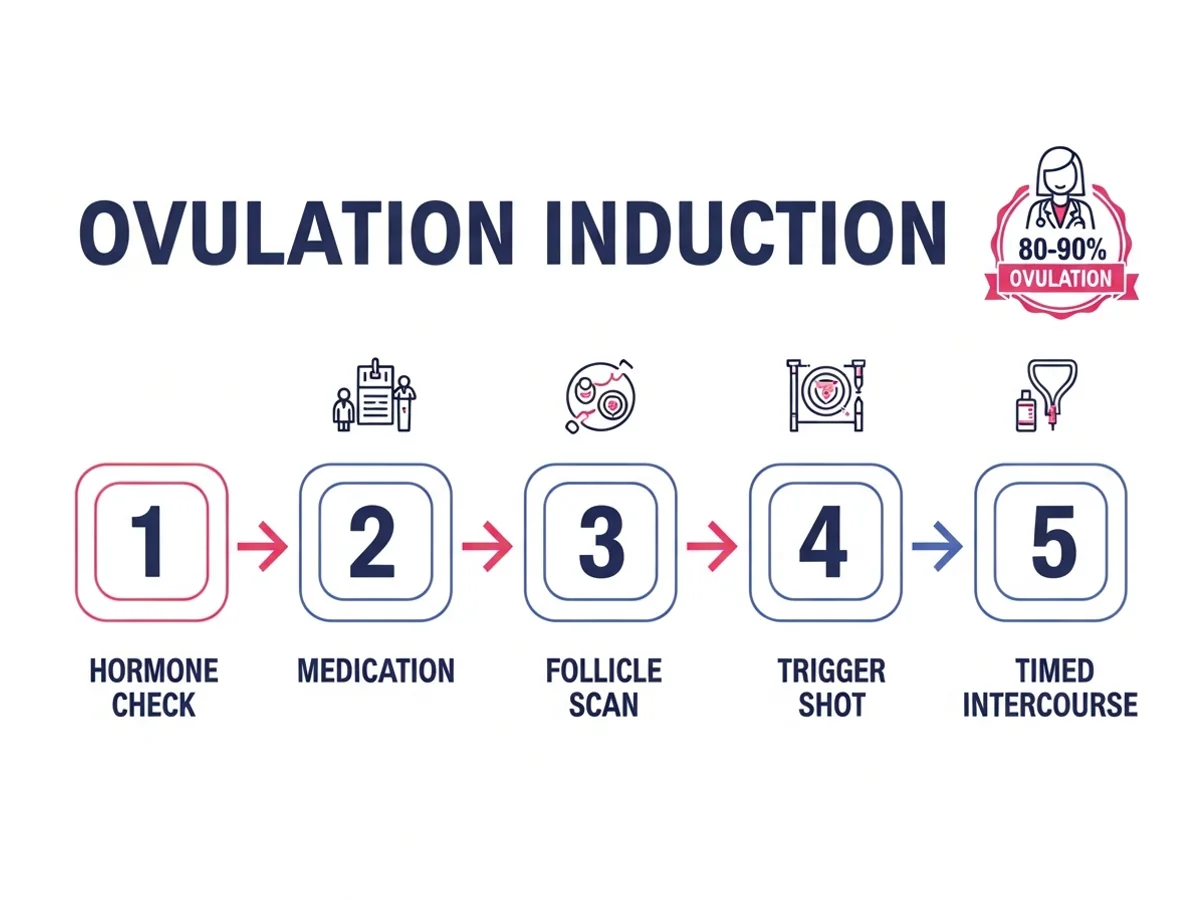
80-90%
Ovulation Achievement Rate
15-20%
Per-Cycle Pregnancy Rate
40-50%
Cumulative Rate (4 Cycles)
When Is Ovulation Induction Recommended?
You should see a specialist if you experience:
- Irregular or absent menstrual periods
- Diagnosed with PCOS or anovulatory cycles
- Unexplained infertility as a first-line treatment approach
- You are preparing for timed intercourse or an IUI cycle
- Previous cycles without ovulation despite lifestyle changes
How Ovulation Induction Restores Your Fertile Cycle
Normal ovulation requires coordinated signals between the brain, pituitary gland, and ovaries. When this axis is disrupted — by PCOS, stress, weight changes, or hormonal imbalance — the ovary fails to develop or release a mature egg. Ovulation induction medications work by either blocking estrogen feedback (clomiphene) or reducing estrogen production (letrozole), both of which stimulate the pituitary to release more FSH. This increased FSH drives follicle growth. Once a follicle reaches 18 to 22 millimetres, ovulation is either triggered with an hCG injection or allowed to occur naturally, creating a defined fertile window for conception.
Conditions We Treat
Ovulation Induction Protocols
Letrozole Protocol
Letrozole (an aromatase inhibitor) is currently the first-line medication for ovulation induction, particularly in PCOS. It typically produces a single dominant follicle with a lower risk of twins compared to clomiphene.
Clomiphene Citrate Protocol
Clomiphene has been used for decades as an effective ovulation inducer. It stimulates FSH release by blocking estrogen receptors. Dr. Rukkayal monitors for multiple follicle development and adjusts doses accordingly.
Low-Dose Gonadotropin Protocol
For patients who do not respond adequately to oral medications, low-dose injectable FSH is administered with careful monitoring. The step-up approach starts with the lowest effective dose to minimise hyperstimulation risk.
Ovulation Induction with Timed Intercourse
Once follicle maturity is confirmed, couples are advised on optimal timing for intercourse. A trigger injection may be used to ensure ovulation occurs within a predictable 36-hour window.
Why Choose Dr. Rukkayal?
- Structured follicular monitoring with every cycle — ovulation medications are never prescribed without ultrasound tracking.
- Protocol selection guided by your specific diagnosis, BMI, and prior treatment response rather than a generic approach.
- Careful dose titration to achieve single follicle development, minimising the risk of twins and ovarian hyperstimulation.
- Honest assessment of when ovulation induction alone is sufficient versus when combining with IUI or stepping up to IVF is warranted.
- PCOS-specific expertise — addressing insulin resistance, weight management, and hormonal optimisation alongside ovulation support.
- Convenient locations across Chennai — Egmore/Chetpet (morning), Mylapore (evening), and Tambaram — plus visiting consultant at Apollo, Motherhood & Cloudnine hospitals.
Your Treatment Journey
Hormonal and Ultrasound Assessment
Baseline blood work (FSH, LH, AMH, thyroid, prolactin) and an ultrasound to assess antral follicle count and rule out ovarian cysts. Dr. Rukkayal identifies the cause of anovulation and selects the appropriate medication.
Medication Start and Dose Selection
Oral medication (letrozole or clomiphene) is started early in your menstrual cycle, typically day 2 to 5. The starting dose is based on your body weight, hormonal profile, and any previous treatment response.
Follicular Monitoring
Serial ultrasound scans from day 9 or 10 track follicle growth and endometrial thickness. Doses are adjusted if the response is too low or too vigorous. The target is one to two mature follicles at 18 to 22 millimetres.
Ovulation Trigger and Timed Conception
When the follicle reaches optimal size, an hCG trigger injection prompts ovulation within 36 hours. You are advised on precise intercourse timing, or IUI is performed if the treatment plan includes insemination.
Luteal Support and Outcome Review
Progesterone supplementation supports the luteal phase. A pregnancy test is performed 14 to 16 days after ovulation. If the cycle is unsuccessful, Dr. Rukkayal reviews the response and adjusts the protocol for the next attempt.

Have Questions About Your Treatment?
Book a consultation with Dr. Rukkayal Fathima to understand your options and next steps.
Frequently Asked Questions
The most common cause is polycystic ovary syndrome (PCOS), which accounts for roughly 80 percent of anovulatory infertility. Other causes include hypothalamic dysfunction from stress or weight changes, high prolactin levels, and thyroid disorders. If you have irregular or absent periods, you likely are not ovulating consistently and may benefit from ovulation induction.
Current evidence favours letrozole as the first-line choice, especially for PCOS patients. Letrozole produces higher ovulation and pregnancy rates with a lower risk of multiple follicle development and twins. It also has a shorter half-life, clearing the body faster and having less anti-estrogenic effect on the endometrium.
Most pregnancies from ovulation induction occur within the first four to six ovulatory cycles. If you have ovulated regularly with medication for four to six cycles without conceiving, Dr. Rukkayal will discuss adding IUI or transitioning to IVF rather than continuing the same approach indefinitely.
Monitoring ensures that the medication is producing the right number of follicles — ideally one or two. Without monitoring, there is a risk of multiple pregnancies from uncontrolled multi-follicle development. Ultrasound also confirms that ovulation actually occurs and that the endometrial lining is developing appropriately for implantation.
With proper monitoring and dose control, the twin rate with letrozole is approximately 5 to 7 percent — only slightly above the natural rate. Clomiphene carries a slightly higher twin risk of 8 to 10 percent. Dr. Rukkayal will cancel the cycle or advise barrier contraception if too many follicles develop, prioritising your safety.
Yes — ovulation induction is the primary treatment for PCOS-related infertility. Letrozole is particularly effective in PCOS, with ovulation rates of 60 to 80 percent and pregnancy rates comparable to more invasive treatments. Addressing insulin resistance and optimising weight before starting medication further improves outcomes.
If letrozole and clomiphene do not produce adequate follicle growth, low-dose injectable gonadotropins are the next step. These require more intensive monitoring but can effectively induce ovulation in resistant cases. If injectable medications also fail, ovarian drilling or IVF may be considered.
Common side effects include mild hot flashes, headache, and occasional mood changes. Letrozole tends to have fewer side effects than clomiphene. Serious complications like ovarian hyperstimulation are rare with oral medications and careful monitoring. Dr. Rukkayal discusses all potential side effects before starting treatment.
Related Specialties
IUI Treatment
Often combined with ovulation induction to further improve conception chances through timed insemination.
Female Fertility
Comprehensive evaluation of all female fertility factors including ovulation, tubal, and uterine health.
PCOS Treatment
Holistic management of polycystic ovary syndrome — the most common cause of anovulatory infertility.
Related Articles
Follicular Study Next Steps
Understand what happens after a follicular study in Chennai. Learn about IUI, IVF, and monitoring with Dr. Rukkayal.
8 min read
Clomid vs Letrozole: Ovulation Boost?
Clomid vs Letrozole for ovulation induction in Chennai? Understand the differences, success rates, and side effects. Consult Dr. Rukkayal Fathima.
12 min read
Follicular Monitoring: Your Chennai Guide
Learn about follicular monitoring in Chennai: process, benefits, cost, and success rates. Expert guidance from Dr. Rukkayal Fathima.
8 min read
Ovulation Induction: Your Guide
How does ovulation induction help you conceive? Dr. Rukkayal explains the medications, process, and success rates in Chennai.
12 min read
Free Fluid After Follicle Rupture: Timeline
Dr. Rukkayal Fathima, fertility specialist in Chennai, explains how long free fluid lasts after follicle rupture, what is normal, and when to worry.
10 min read
PCOS & Fertility in Chennai: Causes & Treatment
How does PCOS affect fertility? Dr. Rukkayal explains the causes, symptoms, and treatment options for women in Chennai.
12 min read
How to Calculate Your Fertile Window Accurately
Learn how to calculate your fertile window for the best chance of pregnancy. Dr. Rukkayal Fathima, a fertility specialist in Chennai, explains methods to find your most fertile days.
9 min read
How to Know If You Are Ovulating for Fertility
Learn how to know if you are ovulating with expert insights from Dr. Rukkayal Fathima, your trusted fertility specialist in Chennai.
9 min read
Ready to Get Started?
Book a consultation with Dr. Rukkayal Fathima about your treatment options
Book AppointmentBook Consultation
Consultation Booked!
Thank you for reaching out. Our team will contact you shortly to confirm your appointment.
Need urgent help? Call us